Foot
The foot is an important part of this case because it was here that the problem began, or at least the first noticeable injury became apparent... the first link in the chain!
Foot slaps down
Whilst I was jogging my right foot started to slap down onto the ground. There appeared to be no reason for it, it just slapped down as opposed to letting me place it on the ground.
This is how I represent the pattern of my jogging, and the major pain.
I was jogging in a rhythmic left-right pattern...
left, right;
left, right;
jog, jog;
jog, jog...
... when the pattern changed to...
jog, jog;
jog, jog;
jog, slap;
jog, slap;
jog, slap...
... which, after (or during) the third 'slap', there followed a 'violent, violent, violent pain' from within the lateral side of my right knee. Nothing whatsoever touched it from the outside. I hobbled home... and haven't jogged since then.
However, after the 'violent, violent, violent pain' eased, there was:
-
no pain,
-
no swelling,
-
no bruising,
-
no redness,
-
no anything...
... but after a short while (and who knows why) a slight pain did arise in my right hip?!
This, to me, clearly displays a timeline upon which to base the order in which things happened, and a rough idea of the activity that was occurring at that time. Despite having little information upon which to develop a theory of what happened, there are the start and end points to consider...
-
the problem must have initially occurred before the first 'slap' in order for my foot to be able to slap down,
-
the problem may have occurred at toe-off of the previous step,
-
as my foot slapped down instantenously, there wouldn't have been time for muscles to become weak and lose control without some sort of external intervention,
-
the violent, violent, violent pain must have occurred whilst my foot was fixed on the ground with the third 'slap',
-
it seems that as my foot slapped down on the ground, it went straight into stance phase, omitting the heel phase, and not getting as far as the toe-off phase of gait,
-
the violent, violent, violent pain was the very last problem at the time of the injury.
So it seems to me that, as this slapping occurred instantaneiously, it cannot have been caused by muscles becoming weak from lack of use or incorrect use. They were working one minute and not the next. Clearly something must have happened to cause this transformation. Muscles cannot become weak of their own accord without some external force, such as disease, neurology or physical damage!
I believe that my body has been 'covering' for my ankle such that I have unknowingly adapted my walking / gait as a pain avoidance strategy.
Trauma mechanism in ankle injuries is described and illustrated with diagrams and x-rays here:
http://www.radiologyassistant.nl/en/p4b6d817d8fade#i4d0499fbd8eed
Ring of stability in the coronal plane
In some fractures there may even be a proximal fibular fracture - which is not visible on the ankle radiographs - in combination with ligamentous ruptures at the level of the ankle.
This suggests that there may be a proximal fibular fracture in conjunction with a ruptured ligament in the ankle...
NOTE: Just in passing... MRI scans of normal ankle:
http://w-radiology.com/ankle-mri-anatomy.php
MRI of the Ankle: Detailed Anatomy
Flat Feet
http://www.ajronline.org/doi/full/10.2214/AJR.09.4199#_i66
(2010)
Introduction
In addition to ankle impingement sy ndromes, extraarticular soft-tissue and osseous impingements occur lateral to the ankle joint, such as talocalcaneal and calcaneofibular impingements [7]. These impingements are sequelae of flatfoot deformity and hindfoot valgus from a variety of causes such as posterior tibial tendon (PTT) deficiency, rheumatologic disorders, diabetes, calcaneal fractures, and congenital flatfoot [7, 8]...
Extraarticular Impingement Syndromes
Pathophysiology and Clinical Features
Severe flatfoot and hindfoot valgus deformity may present with lateral ankle pain in the region bounded by the anterior fibula and the sinus tarsi [7]. This lateral ankle pain has been attributed to extraarticular lateral hindfoot impingement including talocalcaneal impingement (between the lateral talus and calcaneus) [61] and subfibular impingement (between the calcaneus and fibula) [62–64] (Fig. 12A, 12B, 12C). Lateral hindfoot impingement is believed to be secondary to a lateral shift of weight-bearing forces from the talar dome to the lateral talus and fibula [65] and to talocalcaneal joint subluxation [66]. Talocalcaneal impingement typically occurs before subfibular or combined talocalcaneal–subfibular impingements [9, 10].
There are several causes of lateral hindfoot impingement including PTT dysfunction [67, 68], healed intraarticular calcaneal fractures [69], neuropathic arthropathy [70], and inflammatory arthritides [71]. Clinical presentation varies on the basis of the cause of flatfoot and hindfoot valgus...
Regardless of the initial cause of flatfoot, patients with rigid flatfoot deformity experience decreased range of motion at the midfoot and hindfoot and decreased ankle dorsiflexion [72]. Lateral ankle pain may develop because of lateral hindfoot impingement. With progressive deformity, secondary osteoarthrosis of the subtalar, talonavicular, and calcaneocuboid articulations contribute to pain symptoms [62]. On physical examination, flatfoot and hindfoot valgus deformity are evaluated with the patient sitting and standing. There may be decreased range of motion of the ankle, hindfoot, midfoot, and forefoot and lateral ankle pain on palpation. The Achilles tendon may show contracture and tightness [72].
Achilles tendon
Since the Brisk Walking episodes and the introduction of Gait Training, my ankle has continually been getting worse. The problems became apparent not long after the original injury when I discovered that the Achilles tendon was sore when touched / rubbed. No pain, just a feeling of soreness, like a graze to your knee when you fell as a child. One local consultant described it solely as '... where it joins on...'
Nowadays the Achilles tendon area is continually painful. With my foot at an angle of 90 degrees, it feels like pulling or throbbing, whether I'm sitting, standing or lying. However if my foot is at an acute angle, as if going up a hill or being the trailing foot when going downstairs, it feels like it is ripping apart in short, sharp attacks.
Also the area on the medial side of the ankle at the Achilles tendon is continually painful. This feels like small stabbing feelings. I do wonder if it is related to the tibialis posterior muscle because of its position, and because I cannot stand on tiptoes alone on that foot. Occasionally this stabbing feeling may occur on the lateral side of the Achilles tendon too.
And now there are also pains under my heel, and at both sides of my foot, and also occasionally on the top near where the leg joins. These all appear to be random.
Control of Gluteal muscles
Neuromotor control of gluteal muscles in runners with AT
Hip kinematics are closely linked to foot kinematics via mechanical links and may be associated with increased foot eversion. Several studies have reported increased foot eversion during running in patients with Achilles tendinopathy (AT). Thus, the aim of the study is to compare the activation of the gluteus medius (GMED) and maximus (GMAX) – two muscles that alter hip kinematics – in runners with AT.
The results of the study demonstrate altered neuromuscular control of the GMED and [GMAX] in runners with AT. During running, GMED typically activates before heel strike so as to stabilize the hip and the pelvis. In runners with AT, GMED is activated with a delay, which consequently might affect the kinematics of knee and ankle resulting in rear foot inversion. Similarly, GMAX is activated with a delay and for a shorter duration in runners with AT. GMAX is the primary hip extensor and via a kinetic chain, a decreased hip extension moment might be compensated by an increased ankle plantarflexion moment which could potentially increase the load on the Achilles tendon.
Despite their coexistence, it is still not clear whether these alterations are predisposing factors of AT, a consequence of it or maybe a combination. Therefore, they should be treated carefully.
I am wondering whether I have weakness of the GMED because I am not performing the heel strike process. Does the fact that my foot is slapping down onto the ground straight into stance allow the GMED to atrophy? If this is the case, will walking properly after correction strengthen it?
Sprained ankle
And of course it might be a sprained ankle. The majority of ankle sprains occur during flexion and inversion of the foot are discussed by:
http://www.drallenfanderson.com/ankle/ankle-sprain
The calcaneal fibular ligament ligament runs from the tip of the fibula to the tubercle in the calcaneus. The primary function of the calcaneofibular ligament is to restrain inversion of the calcaneus (heel bone) with respect to the fibula. The calcaneofibular ligament and the anterior talofibular ligament play significant roles in different positions of the ankle. The calcaneofibular ligament is the main lateral stabilizer of the ankle in both neutral position and dorsiflexion. The reason that the anterior talofibular ligament is the most commonly injured of these ligaments is that the majority of the sprains occur during flexion and inversion of the foot. The anterior talolfibular ligament is usually the first to suffer disruption followed by the calcaneofibular ligament and subsequently the posterior talofibular ligament...
The most typical injury mechanism of an ankle sprain is when the body weight lands with the foot in plantar flexion, inversion, and adduction. The bony stability of the ankle is diminished in this position and the anterior talofibular ligament and calcaneofibular ligament absorb the stress.
I know that my body weight landed as my foot slapped down onto the ground.
http://www.wheelessonline.com/ortho/supination_and_pronation_of_foot
- Supination:
- supination of foot is a combination of inward rotation at the ankle, adduction of the hindfoot, inversion of the forefoot, and medial arch elevation;
- subtalar joint supination is 3 planes of motion simultaneously:
- adduction
- inversion
- plantarflexion
- as foot supinates the lateral structures tighten;
- continued supination and adduction force may rupture portions of lateral collateral ligaments or avulse these ligaments from their bony attachment sites on the distal fibula, resulting in an ankle sprain;
http://ajs.sagepub.com/content/18/2/196.short
(Am J Sports Med March 1990vol. 18 no. 2 196-200)
Strain in the anterior talofibular ligament increased when the ankle was moved into greater degrees of plantar flexion, internal rotation, and inversion. Strain in the calcaneofibular ligament increased as the talus was dorsiflexed and inverted. These findings support the concept that the anterior talofibular and calcaneofibular ligaments function together at all positions of ankle flexion to provide lateral ankle stability. We measured maximum strain in the posterior talofibular ligament when the ankle was dorsiflexed and externally rotated. The strain in the anterior and posterior tibiofibular liga ments increased when the ankle was dorsiflexed. Ex ternal rotation increased strain in the anterior tibiofibular ligament and decreased strain in the posterior tibiofib ular ligament.
Based upon strain measurements in the lateral ankle ligaments in various ankle joint positions, we believe the anterior talofibular ligament is most likely to tear if the ankle is inverted in plantar flexion and internally rotated. Theoretically, the calcaneofibular ligament tears primarily in inversion if the ankle is dorsiflexed; the anterior tibiofibular ligament tears in dorsiflexion, especially if combined with external rotation; and the posterior tibiofibular ligament tears with extreme dor siflexion.
I wonder whether I actually sprained my ankle TWICE...
-
with a dorsiflexed foot, resulting in plantar flexion and my foot slapping down,
-
with a plantar flexed foot... resulting in damage elsewhere in my knee... ??????????????????????????????????????
This would make a total of 3 sprains if I include that which occurred post-arthroscopy after Brisk Walking exercises.
Can't stand on tiptoes
I cannot stand on tiptoes nor can I support the weight of my body when attempting to stand on tiptoes with my bad, right foot. Standing on tiptoes is regarded as a necessary exercise when treating Achilles insertion tendinitis as discussed by:
... treating an Achilles insertional tendinitis should involve strengthening the forward-most aspect of the tendon. This can be accomplished by performing a series of eccentric load exercises... with the ankle placed through a full range of motion. It is particularly important to work the Achilles tendon with the ankle maximally plantarflexed (i.e., standing way up on tip toes), as this position places greater amounts of strain on the more frequently damaged anterior aspect of the tendon.
This seems to suggest to me that this is more than just Achilles insertion tendinitis!
Can't stand / walk on my heels
https://informatics.med.nyu.edu/modules/pub/neurosurgery/coordination.html
Walking on heels is the most sensitive way to test for foot dorsiflexion weakness, while walking on toes is the best way to test early foot plantar flexion weakness.
Therefore it seems that I do have dorsiflexion weakness because I cannot walk on my heels... BUT I can't walk on toes either...
THEREFORE BOTH DORSIFLEXION and PLANTAR FLEXION WEAKNESS...
Note: Googling 'walking on heels' assumes this relates to high heeled fashion shoes, so there aren't may applicable references freely available...
Can't stand properly on one leg
I have difficulty standing on just my bad, right leg. When I stand on one foot with my good, left leg, I can feel my toes wriggle to help maintain balance. But this doesn't happen with my bad, right leg. With this leg, all my weight seems to be pressing down over my heel. Basically I am supporting all of my weight using the underneath of my heel to help keep my balance. My toes are not involved at all.
And with one leg stands as part of my physiotherapy programme, I have found that I seem to 'sink' lower and lower. I wonder if this is related to my hip, although everyone says that my hips are fine.
eot


Fig
Photograph with arrowheads showing roughly where the Achilles Tendon was initially sore on touching, but nowadays is continually painful.
Fig
Photograph showing the initial main area of pain around the ankle after brisk walks... where the tibialis posterior muscle is located.
Fig
Diagram, taken from
http://classconnection.s3.amazonaws.com/184/flashcards/1904184/jpg/picture21349622500698.jpg
showing the lateral view of the ankle with the Achilles tendon and applicable ligaments.


Fig
Diagram, taken from
http://salk74.files.wordpress.com/2013/04/sup.jpg
showing the effects of supination / underpronation of the right foot.
http://www.nyuhjdbulletin.org/Permalink.aspx?permalinkId=cf5d57fb-4a14-4f58-a483-81499011833a
(2011)
Acute and Chronic Lateral Ankle Instability in the
Athlete
Biomechanics
The ATFL forms a 47° angle to the sagittal plane and 25° angle to the horizontal plane and is the primary restraint against plantar flexion and internal rotation of the foot.12,14,15
The CFL forms a 133° angle with the fibula and a 104° angle with the ATFL. The CFL is relaxed in plantar flexion and taut in dorsiflexion and thus stabilizes the ankle and prevents talar tilt as the ankle moves from neutral into dorsiflexion.12,14,15
The most common mechanism of injury in lateral ankle
sprains occurs with forced plantar flexion and inversion of the ankle as the body’s center of gravity rolls over the ankle. The ATFL followed by the CFL are the most commonly injured ligaments.
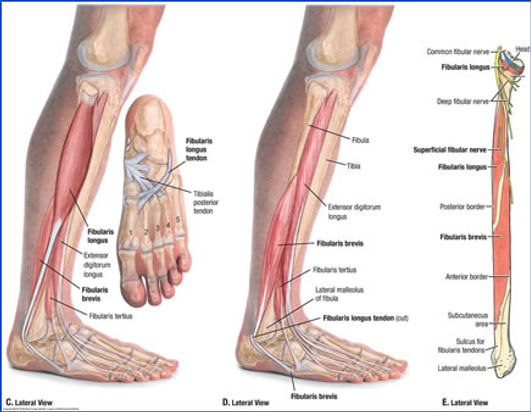
Fig
Diagram of the fibularis / peroneus longus muscle and tendon, and incidently the tibialis posterior tendon beneath the sole of the foot, taken from https://web.duke.edu/anatomy/Lab13-15/lab15images/lab15-step51.jpg

Fig
Photograph showing how the toes on my bad, right leg do not curl up and wriggle around like the toes on my good, left foot.
Fig
Diagram of the extensor digitorum longus muscle used to bend the four small toes upwards. Also to assist in bending the foot at the ankle up toward the body, taken from http://thewellnessdigest.com/extensor-digitorum-longus-pain-in-the-top-of-the-foot/

sot
Not able to wriggle toes
I wish someone would look at the toes on my bad, right foot. They do not curl up and wriggle properly like those on the good, left leg when I am sitting, with my foot leaning on my heel. They are OK when my foot is flat on the floor, just not when I have my foot leaning on the heel. This must indicate a problem with my heel...
Chi Running's Danny Dreyer produced an instructional video on 'How to Avoid Heel Strike' discussed at:
https://www.youtube.com/watch?v=rkUqkdPQHis&feature=share
It seems to me that heel strike is likely to make an impact on the whole leg, and I do wonder whether this was my problem.
Apparently, however, the physiotherapy approach is that, for functional correction therapy, there doesn't appear to be much call for leaning on your heel and wriggling your toes around, so it will not be included for treatment. My concern is more that it is, or might be, indicative of a more substantial problem further up the kinetic chain regarding my lateral knee pain...
And it does appear to be related to the extensor digitorum longus muscle which is used to bend the four small toes upwards and also to assist in bending the foot at the ankle up toward the body. And as the diagram in Fig xxx shows, the extensor digitorum longus muscle runs the whole length between the knee and the foot, connecting the fibular head with the small toes. Surely this must be implicit in my lateral knee pain!
I was booked in for an ultrasound investigation on my right foot but it did not show up any ligament tears, but, as always, I think of questions afterwards.
To me there is clearly a problem with my foot. There are places where it feels sore, like as a child when you fell over and grazed your knees. So, if the ligaments are OK then what else could be causing these issues...? Perhaps there are things that are pulling...? Perhaps ligaments are undamaged, but stretched, or maybe twisted...? Or maybe nerves...?
Fibularis longus
(or peroneus longus muscle)
The extensor digitorum longus muscle is used to bend the four small toes upwards. And also to assist in bending the foot at the ankle up toward the body. It has contact with the fibular at the head and its length. This function seems to be inadequate when I am sitting and leaning on my heel. Perhaps whilst leaning on my heel, something gets compressed such that the extensor digitorum longus muscle is restricted...???
The fibularis / peroneus longus muscle and tendon has contact with the fibular head, its length and the lateral malleolus (the distal or tail end of the fibular) in the ankle.
http://www.sportsinjuryclinic.net/sport-injuries/knee-pain/tibiofibular-joint-dislocation
(On website)
Dislocation of the proximal tibiofibular joint occurs most commonly when the athlete sustains an impact or falls with their knee in a fully flexed position, with their foot pointing inwards (inversion) and downwards. This puts added strain on the muscles which connect the fibula to the foot and toes such as the peroneal muscles. In this position the fibula is pulled forwards and if the force is sufficient it may cause the joint to become dislocated.
This injury should be treated quite seriously as it may sometimes be associated with injury to the peroneal nerve.
It seems to me that my foot is 'pointing inwards (inversion) and downwards' when it 'slaps' down onto the ground when I walk...
I wonder whether damage to the fibularis / peroneus longus tendon, that seems to be placed behind the Achilles tendon, could be responsible for the feeling of soreness on palputation of the Achilles tendon...???